What You Need to Know About the Coming ‘Stealth Omicron’ Wave of COVID-19
Over one million people have already succumbed to COVID-19 in the United States, and current projections suggest that the fifth major wave of the coronavirus could strike at some point in 2022.

COVID-19 claimed its first victim in the United States in early February 2020. On May 16, 2022, the official U.S. death toll passed 1 million—a truly staggering figure by any standard.
What’s more, a statistic known as “excess deaths” indicates that the total number of lives claimed by COVID-19 in the United States could be hundreds of thousands higher than the official number.
Either way, the pandemic has transformed into one of the most tragic events in modern human history, and there’s no clear indication that it will end anytime soon.
New cases in the United States are once again on the rise. And the new culprit appears to be “BA.2,” a subvariant of Omicron which is sometimes referred to as “stealth Omicron.” Like its precursor, BA.2 is extremely contagious, although it’s not believed at this time to be any more deadly than previous strains.
Historical data on case counts and deaths suggests the United States has thus far endured four major waves of the virus. The peaks of those previous waves occurred in April 2020, January 2021, September 2021 and February 2022, as illustrated below.
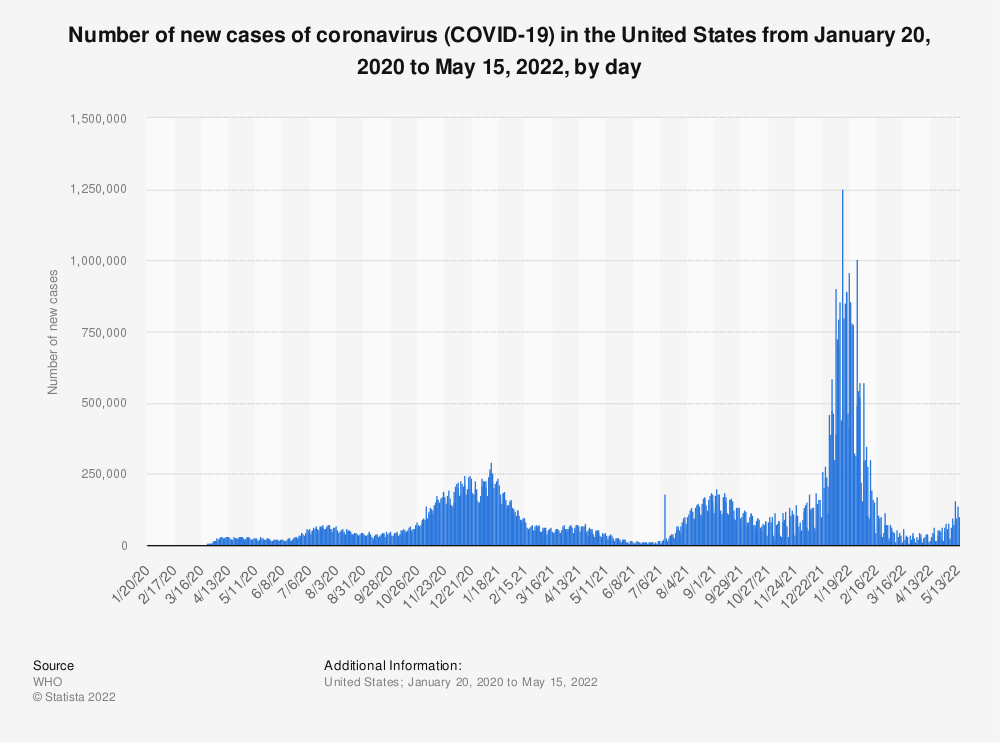
While nothing is certain, most projections suggest that a fifth wave will materialize at some point in 2022. One can only hope that the severity of the oncoming wave is mild, or that it never materializes at all.
COVID-19 vaccine update
Unfortunately, the Omicron variant served to expose the limitations of widespread vaccination. Not because vaccines are ineffective, but because mutations in the virus are shifting too quickly for vaccinologists to effectively keep pace.
So-called breakthrough infections rose sharply during the last Omicron wave, which are defined as infections occurring in vaccinated individuals.
However, data compiled by various sources illustrates that the risk of severe illness, hospitalization and death were reduced significantly in fully vaccinated individuals compared with unvaccinated individuals. The data below—compiled by The Washington Post—illustrates this reality very clearly.

The above highlights how the spread of the Omicron variant appears to have reduced the protections afforded by existing vaccines.
However, one has to acknowledge that this is where the speed of the virus’s mutation plays a big role. Vaccinologists aren’t able to create, test and manufacture modified vaccines at a pace that keeps up with the virus.
Despite those limitations, research continues to support the impact of vaccines and boosters, especially right after a dose is administered. For example, a comprehensive study published by BMC Infectious Diseases found “evidence of immunity against SARS-CoV-2 infection from a high of 83% at one month to 22% at five months or longer after being fully vaccinated.”
Notably, the scientists conducting this study also concluded that for vaccinated individuals, “protection against severe disease remained robust; 90% at five months following vaccination.”
This data is supported by a similar study published by the Centers for Disease Control and Protection (CDC) which concluded that the “receipt of 2 or 3 doses of a COVID-19 mRNA vaccine conferred 90% protection against COVID-19-associated IMV or in-hospital death among adults.”
But to sustain that type of effectiveness, it will be imperative for the biotechnology sector to create and manufacture updated vaccines, as well as to create and deliver new treatments for COVID-19.
These sentiments were echoed by the White House COVID-19 coordinator Dr. Ashish Jha when he indicated on May 12 that the U.S. would become increasingly vulnerable to the coronavirus this fall and winter if Congress doesn’t swiftly approve new funding for new vaccines and treatments.
Forthcoming vaccines are expected to specifically target the Omicron strain (and associated substrains like BA.2) because that particular mutation of the coronavirus has been more adept at circumventing the defenses provided by existing vaccines.
COVID-19 treatment updates
The good news in 2022 is that there are now several different treatments approved by the Food and Drug Administration (FDA) that can be utilized to combat COVID-19 during the initial stages of incubation.
That means human civilization now has more ammunition to protect itself against the virus. The two types of newly approved treatments include monoclonal antibodies and antivirals.
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses, like SARS-CoV-2. Bebtelovimab, made by Eli Lilly (LLY), is currently the only monoclonal antibody treatment that has been granted emergency use authorization (EUA) by the FDA to treat COVID-19.
Authorized in February 2022, the treatment is indicated when “alternative COVID-19 treatment options approved or authorized by the FDA are not accessible or clinically appropriate.” It is typically administered intravenously shortly after symptoms develop. This treatment has been shown to be active against the omicron variant.
It should be noted that efficacy data from placebo-controlled trials that evaluated the use of Bebtelovimab in patients who are at high risk of progressing to severe COVID-19 isn’t available, which is why Bebtelovimab is only recommended when the preferred treatment options are not available, feasible to use or clinically appropriate.
Antiviral drugs are a class of medication used for treating viral infections. Unlike antibiotics, antiviral drugs do not destroy the target pathogen; instead, they are designed to inhibit its development.
At present, there are two antivirals that were recently approved by the FDA for the treatment of COVID-19: Paxlovid and Molnupiravir.
Paxlovid, made by Pfizer (PFE), was approved for use in December 2021 for the treatment of mild-to-moderate COVID-19 in people at least 12 years of age who are at increased risk for severe illness. This treatment is available by prescription only, after a positive COVID-19 test and within five days of symptom onset.
In a study conducted by Pfizer, results showed that those who had taken Paxlovid within five days of the start of symptoms had an 88% reduced risk of COVID-related hospitalization or death compared to placebo.
Paxlovid is not authorized to prevent infection, to prevent illness after exposure (prior to diagnosis), or to treat someone hospitalized with severe COVID-19.
Last December, the FDA also authorized Molnupiravir, an oral antiviral treatment manufactured by Merck (MRK), for the treatment of mild-to-moderate COVID-19 in people at least 18 years of age who are at an increased risk of severe illness. Much like Paxlovid, the treatment is available by prescription only, after a positive COVID-19 test and within five days of symptom onset.
Similar to Paxlovid, Molnupiravir is indicated when other COVID-19 treatments “are not accessible or clinically appropriate.”
Unfortunately, the efficacy data stemming from clinical trials for this particular treatment demonstrated that Molnupiravir only reduced the risk of hospitalization and death by 30% in people with mild or moderate COVID-19 who were at high risk for severe COVID. According to that data, its potency is reduced compared with Paxlovid.
For hospitalized patients, the treatment regiment varies, but some common approaches include supplemental oxygen, ventilation, Remdesivir and Dexamethasone. Remdesivir is an antiviral that was originally created as a potential treatment for hepatitis. Dexamethasone is a type of steroid and provides assistance in tempering the body’s immune response.
Another medication, known as Tocilizumab, may also be administered in certain severe cases. This drug was originally created to treat rheumatoid arthritis.
Those seeking a prescription treatment for COVID-19 can contact their doctor, and may also want to visit the “Test to Treat” website. Test to Treat is a government initiative that makes it faster and easier for people with COVID-19 to obtain treatment, including antivirals.
To follow everything moving the financial markets this summer, readers can tune into TASTYTRADE LIVE at their convenience.
This post is for informational purposes only and does not represent medical advice. Readers seeking medical advice should contact a medical professional.
Get Luckbox! Subscribe to receive 10-issues of Luckbox in print! See SUBSCRIBE or UPGRADE TO PRINT (upper right) for more info or visit getluckbox.com.
Sage Anderson is a pseudonym. He’s an experienced trader of equity derivatives and has managed volatility-based portfolios as a former prop trading firm employee. He’s not an employee of Luckbox, tastytrade or any affiliated companies. Readers can direct questions about this blog or other trading-related subjects, to support@luckboxmagazine.com.